
PCOS is one of the most common female endocrine disorders. PCOS is a complex,
heterogeneous disorder of uncertain etiology. Both genes and the environment
contribute to PCOS. Obesity, exacerbated by poor dietary choices and physical
inactivity, worsens PCOS in susceptible individuals.
PCOS produces symptoms in approximately 5% to 10% of women of reproductive age
(12–45 years old). It is thought to be one of the leading causes of female
subfertility and the most frequent endocrine problem in women of reproductive
age.
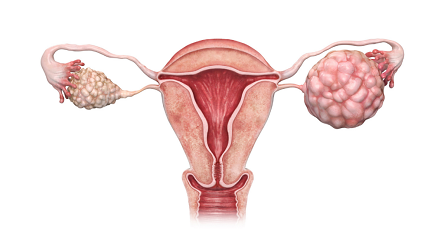
The principal features are anovulation, resulting in irregular menstruation,
amenorrhea, ovulation-related infertility, and polycystic ovaries; excessive
amounts or effects of androgenic hormones, resulting in acne and hirsutism; and
insulin resistance, often associated with obesity, Type 2 diabetes, and high
cholesterol levels.[8] The symptoms and severity of the syndrome vary greatly
among affected women.
PCOS includes a heterogeneous collection of signs and symptoms with varying degree of mildness and severity in affecting the reproductive, endocrine and metabolic functions.The classic triad of the disorder includes hirsutism, menstrual dysfunction, and obesity. Some common symptoms of PCOS include:
Menstrual disorders: PCOS mostly produces oligomenorrhea or amenorrhea, but other types of menstrual disorders may also occur.
Infertility:This generally results directly from chronic anovulation (lack of ovulation).
Hyperandrogenism: The most common signs are acne and hirsutism (male pattern of hair growth), but it may produce hypermenorrhea (very frequent menstrual periods) or other symptoms.Approximately three-quarters of patients with PCOS (by the diagnostic criteria of NIH/NICHD 1990) have evidence of hyperandrogenemia.
Metabolic syndrome: This appears as a tendency towards central obesity and other symptoms associated with insulin resistance. Serum insulin, insulin resistance andhomocysteine levels are higher in women with PCOS.
When comparing success rates of different clinics, it is important to know what type of pregnancies are being compared. A chemical pregnancy is one confirmed by blood or urine tests, but in a clinical pregnancy where pregnancies are typically verfied through ultrasound, a miscarriage may occur before the pregnancy can be confirmed. After a clinical pregnancy has been verified, a miscarriage may still occur, but it is less likely.
PCOS is a complex, heterogeneous disorder of uncertain aetiology. Both
genes and the environment contribute to PCOS. Obesity, exacerbated by
poor dietary choices and physical inactivity, worsens PCOS in
susceptible individuals. There is strong evidence that there is a
genetic component in many cases. Such evidence includes the familial
clustering of cases, greater concordance in monozygotic compared with
dizygotic twins and heritability of endocrine and metabolic features of
PCOS.
The genetic component appears to be inherited in an autosomal dominant
fashion with high genetic penetrance but variable expressivity in
females; this means that each child has a 50% chance of inheriting the
predisposing genetic variant(s) from a parent, and if a daughter
receives the variant(s), then the daughter will have the disease to some
extent. The genetic variant(s) can be inherited from either the father
or the mother, and can be passed along to both sons (who may be
asymptomatic carriers or may have symptoms such as early baldness and/or
excessive hair) and daughters, who will show signs of PCOS. The allele
appears to manifest itself at least partially via heightened androgen
levels secreted by ovarian follicle theca cells from women with the
allele. The exact gene affected has not yet been identified.
The clinical severity of PCOS symptoms appears to be largely determined
by factors such as obesity.